
Everything you need to know after a scapula fracture
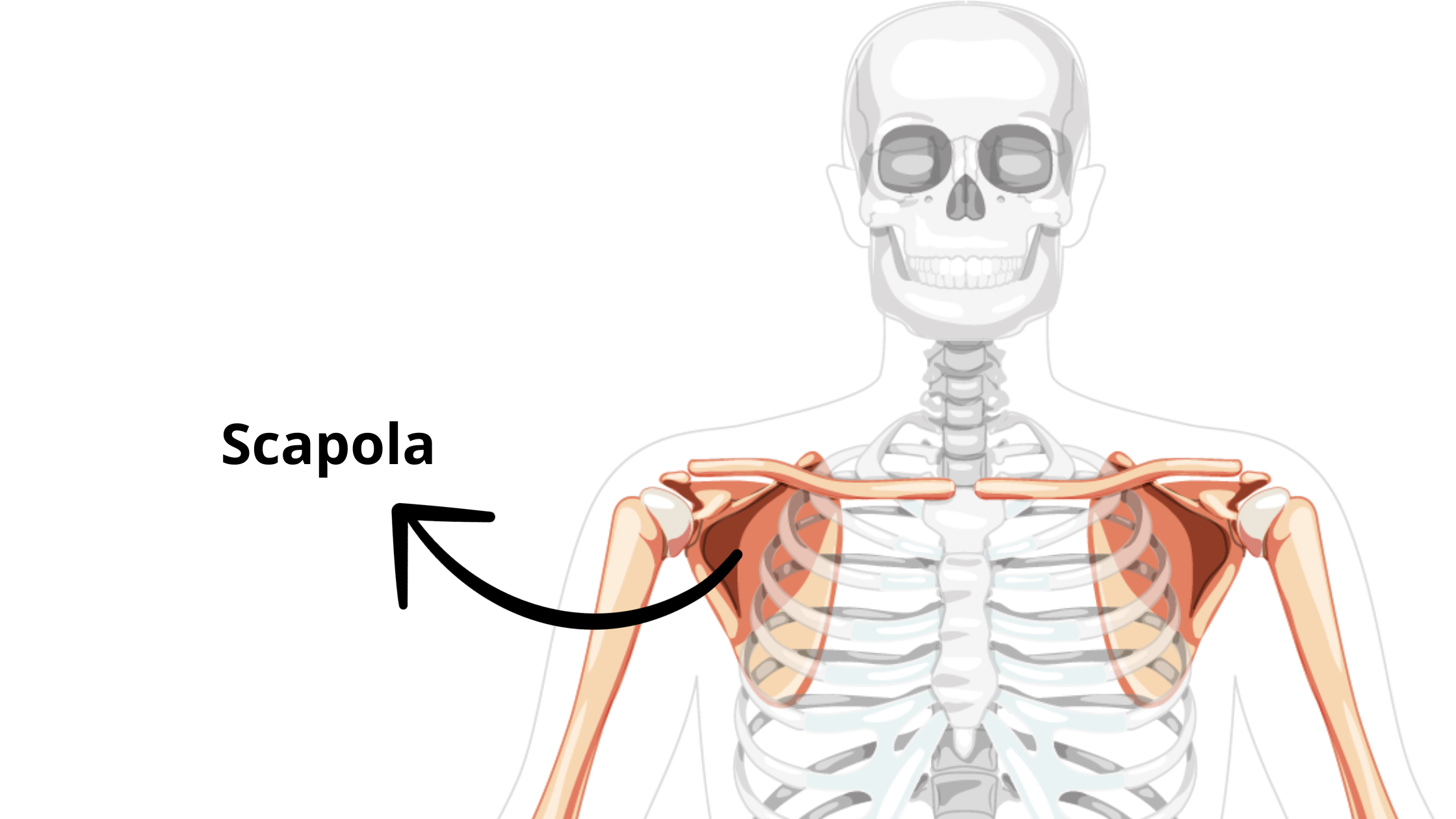
The scapula is a flat and triangular also known as the shoulder blade.
It connects the upper limb to the trunk and articulates the humerus at the gleno-humeral joint and with the clavicle at the acromioclavicular joint.
The costal surface of the scapula faces the ribcage.
You can feel the spine of the scapula by placing a hand on your opposite shoulder, sliding inward.
If you know someone who often suffers from neck pain, especially on one side only, they will automatically put a hand on the painful area, trying to alleviate the symptoms.


The scapula bone is anteriorly composed by:
- Acromion: the protruding bony tip that you can easily palpate on both shoulders;
- Glena (glenoid): this cavity forms the gleno-humeral joint along with the humerus and it's where the articular cartilage lies,
- Coracoid process: is a small hook-like structure on the lateral edge of the superior anterior portion of the scapula and from it some muscles, such as the short head of the biceps brachii originates.

And is subsequently composed by:
- Scapula spine: divides the scapula into two distinct areas, the infraspinatus fossa and the supraspinatus fossa. Its extension forms the acromion;
- Infraspinatus fossa: area of origin of some muscles that are part of the "rotator cuff muscles";
- Supraspinatus fossa: area of origin of the supraspinatus muscle (or also called supraspinatus), famous for frequent injuries due to repeated movements over time.

The main movements that the scapula allows are:
- Arm flexion and extension:

- Arm adduction and abduction:

- External and internal rotation of the arm (also elbowed at 90°):

An high intensity trauma is the main cause of scapular fractures, with also other collateral damage, such as rib fractures, vertebral fractures, contusions, etc. (called polytrauma).
The mechanism of injury is caused by a direct blow - the fall of a heavy object on the shoulder blade from great heights - as happens during car accidents, sports and work traumas.

Similar to clavicle fractures, you may experience:
- Sharp pain;
- Swelling around the shoulder and posterior compartment;
- Bone deformity;
- Ecchymosis (blood extravasation under the skin);
- Closure attitude of the damaged shoulder and the arm in contact with the chest, in a defensive position, supported by the hand of the opposite limb;
- Very painful movements of the shoulder, especially if you try to lift the arm outwards;
- Abrasions of the skin, due to friction with possible surfaces, such as in the case of road accidents, falls, etc.

Fractures of the scapula are classified based on their anatomical location:
- Fracture of the body of the scapula
- Fracture of the glenoid rim and articular surface
- Fracture of the neck of the scapula
- Fracture of the coracoid process
- Fracture of the acromion
- Fracture of the spine of the scapula

The diagnosis of scapula fracture is obtained thanks to a radiographic examination, which includes various projections, including the antero-posterior and the lateral, from the axillary section.
A double projection allows the radiologist to diagnose particular fractures that go unnoticed and be classified as false positives.
The use of computed tomography is almost always necessary to diagnose fractures of the glenoid and neck of the scapula.
Magnetic resonance imaging allows us to observe possible lesions associated with the muscle and tendon tissues of the entire shoulder girdle, especially in high-intensity trauma.

In both compound and displaced fractures, a brace is applied in the arm pocket, consequently the best positions for sleeping, in order of importance and comfort, are:
- Supine in a reclined position (in this position the weight of the body does not get worse fully on the shoulder blade, with the risk of pain). The further you go with the treatment, the more you will be able to recline further the backrest;
- Fetal position (naturally on the healthy side);
- Lying on your stomach (if you don't feel pain), especially if you don't have a bench or a reclining chair available, then you can create a wall of pillows to support your back.
The only not recommended position, as an addition to sleeping on the "sick" side, is to lie on your stomach.
This position is quite complicated, not only because the brace must be kept all night, until the doctor tells you that you can remove it, but also because the tension on the shoulders could increase and cause joint and muscle pain in the shoulder and neck.
